Clinical Aspects of Liver Diseases
4
0
Tr
eat
m
e
n
tof
liv
e
r
d
i
seases
Pa
g
e:
1
From m
y
tholo
gy
to
p
rovable treatment
8
72
1
.1 In
g
lobal medicine
8
72
1
.2 In hepatolog
y
8
72
2
C
linical studies
8
73
2
.1 T
yp
es of clinical studies
8
73
2
.2 Problems of clinical studies
8
73
2
.3 Placebo
8
74
2
.4 D
i
ff
i
culty of evaluat
i
on
8
74
2
.5 Provabilit
y
of treatmen
t
8
74
3
Pr
i
nc
ipl
es o
fli
ver t
h
era
py
8
75
3.1 Bas
i
c cons
i
derat
i
ons
8
75
3.1.1 L
i
ver therap
y
8
75
3.1.2 Liver thera
p
eutic a
g
ents
8
75
3.1.3 Protective thera
py
of the live
r
8
75
3.2 Precond
i
t
i
ons
8
75
3.3 Formsof“l
i
ver therapy
”
8
76
3
.
4 Aim
so
f
t
r
eat
m
e
n
t
8
76
3.5 Cate
g
ories of “liver thera
p
eutics” 876
3.6 Act
i
ve substances
8
7
6
3.7 Dose adjustment of medicaments 87
7
3.8 Si
g
nificance of
q
ualit
y
of life
8
7
8
3.9 Assessment of survival rate
8
7
8
4
Nutr
i
t
i
ona
l
t
h
erapy o
fli
ver
di
sease
s
8
7
8
4.1 Artificial feedin
g
8
79
4.1.1 Enteral feedin
g
8
79
4.1.2 Parenteral feed
i
n
g
8
7
9
4.2 D
i
et
i
n malnutr
i
t
i
o
n
880
4.3 Special diet
s
8
8
0
5
Dru
g
t
h
era
py
o
fli
ver
di
seases
881
5.
1
V
irustatics
881
5.1.1 Interfero
n
8
82
5.1.2 Nucleoside analogues
8
83
5
.2
I
mmunosu
pp
ressants
88
4
5.2.1 Glucocort
i
co
i
ds
88
4
5.2.2 Azath
i
opr
i
n
e
8
84
5.2.3 Cyclosporine
A
8
85
5
.
2
.
4T
ac
r
o
lim
us
88
5
5.2.5 C
y
clo
p
hos
p
ham
i
de
88
5
5.2.6 Methotrexate
8
85
5
.3
I
mmunostimulant
s
8
85
5.3.1
S
eleniu
m
88
5
5.3.2 Z
i
nc
886
5.3.3 Thymos
in
8
86
5
.4
U
rsodeox
y
cholic aci
d
8
86
5
.5
L
actulose
887
8
7
1
Pa
g
e
:
5
.6
Br
anched
-
chain amino acids
888
5
.7
Amino acids o
f
the urea c
y
cle 89
0
5
.8
D-
p
enici
ll
amin
e
892
5.
9
Somatostati
n
892
5.10 Terlipressin 89
2
5
.
11 S-adenos
y
l-L-methionine 89
3
5
.12
H
aemar
g
inate
893
5.
1
3 P
h
ytot
h
erapeutics
894
5.13.1 Essent
i
al phosphol
i
p
i
d
s
89
4
5.13.2 Silymarin 89
6
5.13.3 Gl
y
c
y
rrhiza
g
labr
a
89
7
5.13.4 Colch
i
c
i
n
e
89
7
5.13.5 Beta
i
n
e
897
5.13.6 Cynara scolymu
s
898
5.13.7 Bu
pl
eurum
f
a
l
catu
m
898
5.13.8 P
hyll
ant
h
us amaru
s
898
5.13.9 Sch
i
zandra ch
i
nens
i
s 898
5.13.10
C
atechin 898
6
S
ur
gi
ca
l
t
h
era
py
o
fli
ver
di
seases
898
6
.
1
TIPS
899
6
.2 Shunt operatio
n
899
6.
3 Block surger
y
9
0
0
6.
4
Live
rr
esection
900
6
.4.1 Bas
i
c
p
r
i
nc
ip
le
s
900
6
.4.2 Class
i
f
i
cat
i
on and
i
nd
i
cat
i
ons
9
01
6
.4.3 Re
g
eneration
9
0
2
6.
5
L
iver in
j
urie
s
902
7
Li
ver trans
pl
antat
i
o
n
903
7.1 Ind
i
cat
i
ons
9
0
3
7.2
C
ontraindications
9
0
5
7.3 Preo
p
erative dia
g
nostics
905
7.4 Preparat
i
on of pat
i
ents
906
7.5 Surg
i
cal aspects
9
0
6
7.6 Posto
p
erative feature
s
9
0
8
7
.
7Af
te
r
ca
r
ea
n
d
r
e
h
ab
ili
tat
i
o
n
910
8
S
oc
i
ome
di
ca
l
aspect
s
911
8.1 Health awareness
9
11
8
.
2Pr
e
v
e
n
t
iv
e
m
ed
i
c
in
e
9
1
2
8
.
3R
e
h
ab
ili
tat
i
on
912
8.4 Capac
i
ty for wor
k
912
8.5 Self-help group
s
9
1
4
앫
R
e
f
erences
(
1
⫺
4
45
)
9
1
4
(
Fi
g
ures 40.1
⫺
4
0.11; ta
bl
es 40.1
⫺
40.19
)
4
0
Tr
eat
m
e
n
tof
liv
e
r
d
i
seases
1
From mythology to provabl
e
t
r
eat
m
e
n
t
1.1 In
g
lobal medicine
䉴
Reco
mm
e
n
dat
i
o
n
sa
n
dd
i
scuss
i
o
n
so
n
t
h
et
r
eat-
m
ent of d
i
seases and
i
n
j
ur
i
es are as old as med
i
c
i
ne
i
tself. Accord
i
ng to our knowledge of earl
i
er t
i
mes
,
m
edicine has its origins i
n
m
ythological therapy
.
Thi
s
a
lso a
pp
lies to the treatment of liver diseases. •
U
n
d
erstan
d
a
bly,
“
surgica
l
me
d
icine
”
,es
p
ec
i
all
y
trau-
m
atology, en
j
oyed the h
i
ghest sc
i
ent
i
f
i
c status
in
a
ntiquity, since the actual “cause” and medical
“effect” were most obvious in this field. • M
y
tho
-
l
o
gi
cal
i
deas and r
i
tuals were therefore of m
i
nor s
ig
-
ni
f
i
cance to the barber surgeon:
i
n general, pract
i
cal
experience, manual skill and (mostly self-developed
)
app
ro
p
riate instruments
p
roduced the desired result
.
By
contrast,
“conse
r
vative medicine”
was c
h
arac-
ter
i
zed by mythology, steeped
i
nr
i
tual as well as
(mantic) divination and, for many epochs, mostly left
in the hands of the “
p
riest doctor”. In s
p
ite of some
-
t
i
mes aston
i
sh
i
n
g
l
yg
ood d
i
a
g
nost
i
cca
p
ab
i
l
i
t
i
es and
p
rognost
i
c accuracy, med
i
c
i
ne on the whol
e
⫺
espe-
c
ially treatment of the individual patien
t
⫺
was sub-
j
ect to the
p
revailin
g
m
y
tholo
gy
of the res
p
ectiv
e
e
p
oc
h
.
(
s. ta
b
. 40.1
)
W
ith the
g
radual re
j
ection of “m
y
thos” and a
s
tronger tendency to “logos”, therapeut
i
c measures
of a mytholog
i
cal and r
i
tual nature were
i
ncreas
i
ngly
a
bandoned. At the same time
,
h
o
wever, the a
bsu
r
d
a
ideas o
f s
p
eculat
i
ve thera
py
reached an unima
g
inable
l
evelofod
i
ousness. Obscure m
i
xtures, fantast
i
c prep-
a
rat
i
ons as well as nauseat
i
ng and even cruel treat
-
m
ent met
h
o
d
s were more an
d
more
p
ro
p
a
g
ate
d
an
d
app
lied. An insi
g
ht into these abnormalities of s
p
ecu
-
l
at
i
ve med
i
c
i
ne
i
sg
i
ven b
y
K.F. Paullin
i
(
1699
)
in hi
s
book:
„Neu-verme
h
rte,
h
ei
l
same Drec
k
-A
p
ot
h
e
k
e
“
(“Rev
i
sed and Enlarged Curat
i
ve D
i
rty Pharmacy”)
.
Wi
th the com
i
n
g
of the A
g
e of Enl
ig
htenment
i
n the
mi
ddle of the 18
t
h
centur
y
, accom
p
anied b
y
ara
p
i
d
i
ncrease
i
n med
i
cal knowledge, the calls for con
-
fi
rmed results became more and more urgent. Th
i
s
led to the ad
v
e
n
tof
em
p
irical thera
py
, which required
y
y
s
ubtle observation, critical anal
y
sis, careful examin
-
a
t
i
on and, above all, a wr
i
tten record of case h
i
stor
i
es
.
I
nth
i
s connect
i
on, surg
i
cal emp
i
r
i
c
i
sm was mor
e
s
tron
g
l
y
based on mor
p
holo
g
ical facts and ob
j
ectiv
e
m
ethodolo
g
ical ex
p
erience than the thera
p
eutic
emp
i
r
i
c
i
sm of conservat
i
ve med
i
c
i
ne
.
8
7
2
䉴
P
reventive thera
p
eutic em
p
iricism was a
pp
lied fo
r
t
he first time around 1600, when it was discovered b
y
“
thera
py
com
p
ar
i
son” that those seamen of the Eas
t
Ind
i
a Company who drank lemon
j
u
i
ce as a supple
-
m
entar
y
bevera
g
e did not contract scurv
y.
T
his was
th
e
b
asis o
f(
pro
b
a
bly)
t
h
e
f
irst
“
stat
i
st
i
ca
l”
t
h
era
p
eu-
ti
c stu
dy,
which
J
.
L
IN
D carried out in 17
4
7inordert
o
con
f
irm t
h
et
h
eor
y
o
f
a
l
emon-
j
uice t
h
erap
y
in severa
l
groups o
f
peop
l
e
b
ya
d
ministering various su
b
stances,
i
ncluding a “placebo”
.
T
h
i
s theory was also conf
i
rmed
b
y
J. C
oo
k in 1776, usin
g
a similar stud
y
desi
g
n.
•
F
urther therapeut
i
cm
i
lestones of med
i
cal h
i
stor
y
i
nclude the comparat
i
ve stud
i
es w
i
th digitalis
(W.
W
itherin
g
,
1785
)
,
s
mallpox vaccine
(
E.
J
enner
, 1798)
rr
a
n
d
m
ercur
y
treatment of syphilis
(
J.
P
earson
,
1800
)
.•
S
uch
com
p
arative studies, which were based on individua
l
o
bservations, aimed at
p
rovin
g
the effectiveness of
t
reatments; th
i
s development ended the epoch o
f
e
mp
i
r
i
cal therapy.
(2
)
(
ta
b
. 40.1
)
1
.2 In he
p
atolo
gy
䉴
D
ur
i
ng a per
i
od of about 3,000 years, hepatology als
o
e
xper
i
enced thes
e
historical medical epochs of therapy
,
(
1
.) mythological, (
2
(
(
.
)
s
p
eculative,
(
3
.)
em
p
irical, and
(
4
.) p
rovable.
(
s. tab. 40.1
)
• In addition to cata
p
lasm
s
⫺
c
ons
i
st
i
ng of var
i
ous herbs, o
i
ls or products der
i
ve
d
from an
i
mals, mostly prepared and used accord
i
ng t
o
m
y
tholo
g
icall
y
related idea
s
⫺
c
u
pp
in
g
, scarification
,
e
nemas, blood-lettin
g
and sternutators, the followin
g
mater
i
als were also used: dr
i
ed wolf l
i
ver w
i
th honey,
donkey l
i
ver w
i
th parsley, raw ox l
i
ver d
i
pped
i
n honey
,
o
x blood, etc. Some hi
g
hl
y
com
p
lex and fantasti
c
m
y
tholo
g
ical diets were a
pp
lied as well. Thera
p
euti
c
measures were often based on certa
i
n mytholog
i
ca
l
numbers or r
i
tual-dependent po
i
nts
i
nt
i
me and per
-
formed before statues of
g
ods or in connection with ani-
mal sacrifice
.
(
see c
h
a
p
ter 1.
)
• From the mediaeval
“d
i
rty pharmacy” came numerous, d
i
sgust
i
ng therapeu-
t
ic recommendations for patients with liver disease, e.g
.
consum
p
tion of the excrement of certain animals, ea
r
w
ax, dirt scra
p
ed off shee
p
udders, earthworms,
p
ol
y
-
pods d
i
ssolved
i
nw
i
ne, or a certa
i
n number of l
i
v
e
sheep’s lice. (s. p. 446) • Empirical treatment increasingl
y
made use of substrates of
p
lant ori
g
in or extracts o
f
Hy
oscamus, Cheliodonium, dandelion or milk thistle,
e
tc. To my knowledge, comparative therapeutic investiga-
ti
on
s
such as those mentioned above were not performe
d
in he
p
atolo
gy
. Until modern times, treatment of live
r
d
i
seases rema
i
ned almost exclus
i
vel
y
em
pi
r
i
cal
⫺
a
n
d
t
hus sc
i
ent
i
f
i
cally unproven.
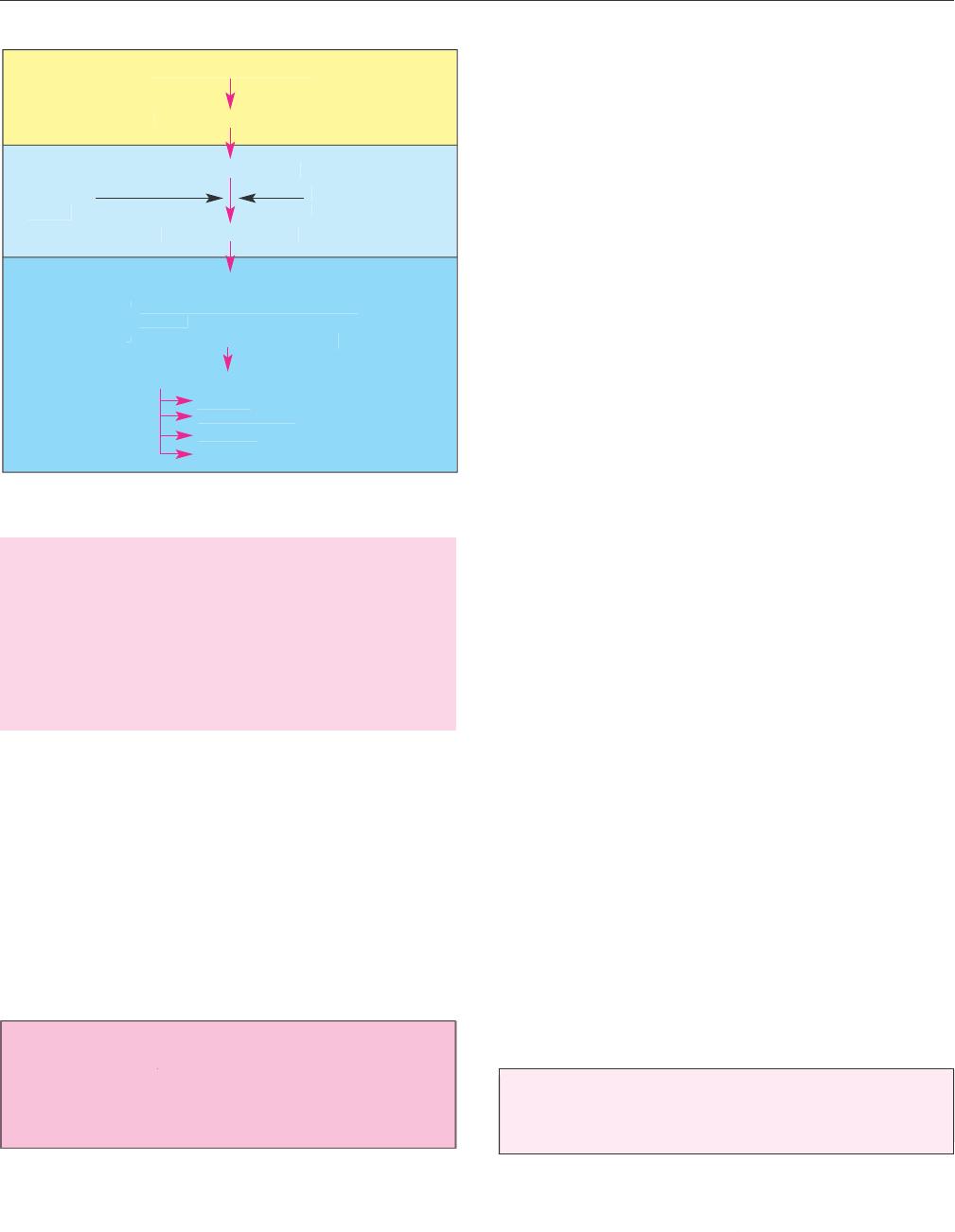
Treatment o
fl
iver
d
isease
s
M
y
tholo
g
ical therap
y
S
peculative therap
y
Emp
i
r
i
cal therap
y
La
c
k
o
f
T
hera
p
euti
c
p
roof
n
ihili
s
m
A
d
j
uvant therap
y
P
r
ov
a
b
l
e
tr
e
atm
e
n
t
•
p
h
armaco
l
og
i
ca
l
exper
i
menta
l
s
t
ud
i
es
•
clinicall
y
controlled studie
s
New approaches to treatment
g
enet
ic
bio
m
olecula
r
i
nvas
i
v
e
sur
g
ica
l
Tab. 40.1:
E
pochs of medicine:
(
1
.) mythological, (
2
(
(
.
) speculative
,
a
nd
(
3
.) emp
i
r
i
cal therapy, through to (
4
.) provable treatmen
t
The occas
i
onally pronounced “polypragmatism”
was
c
onfronted by the opposite extreme o
f
“
therapeuti
c
n
i
h
i
l
is
m
”
i
n the sense of treatment based on ex
p
ect-
a
t
i
on. Th
i
s
i
nev
i
tabl
y
led to frustrat
i
on on the
p
art o
f
t
he phys
i
c
i
an and to res
i
gnat
i
on on the part of the
patient suffering from a liver disease. • Thus, the real
-
i
zation of
p
rovable treatment also became an ur
g
en
t
c
hallen
g
e
i
nhe
p
atolo
gy.
2
Clinical studie
s
䉴 The f
i
rst eth
i
cal pr
i
nc
i
ples of b
i
omed
i
cal research ha
d
alread
y
been develo
p
ed in German
yp
rior to World
War I: relevant instructions were issued b
y
the Prussia
n
E
ducat
i
on Off
i
ce
i
n 1900. • At the proposal of the Ger
-
man Nat
i
onal Health Board, gu
i
del
i
nes for modern
curative treatment and for the
p
erformance of scientifi
c
studies in humans were issued in 1931 b
y
the Ministr
y
o
f Internal Affa
i
rs
i
n Germany.
Th
i
s measure was
i
ndeed the beg
i
nn
i
ng of scienti
f
ic
-
ally based therapy
.
• In 193
2
y
y
P
.M
artini
published hi
s
methodolo
gy
of thera
p
eutic research
(
8
)
,
and in 193
7
A.B. H
ill
established the
p
rinci
p
les of medical statis-
ti
cs
.
(6
)
2.1 Types of clinical studies
S
i
gn
i
f
i
cant contr
i
but
i
ons have s
i
nce been made concern
-
i
n
g
the im
p
ortance,
p
erformance and evaluation of
c
lin
-
ica
l
studies.
(
5, 7
)
In recent
y
ears, statistical and le
g
al
issues in
p
articular have been discussed
.
(
3, 10, 11, 12
)
•
C
ontrolled cl
i
n
i
cal stud
i
es are r
ig
htl
y
called for and the
y
8
73
are
i
nd
i
spensable for avo
i
d
i
ng therapeut
i
cm
i
s
j
udgement
deriving from “trial and error” and for creating a
n
ob
j
ective basis for official decisions. The
y
ma
y
be car
-
ri
ed out, as far as
p
oss
i
ble com
p
arat
i
vel
y
, as a retros
p
ec-
t
i
ve or prospect
i
ve
i
nvest
i
gat
i
on. • A retrospective study
is a backward-looking review of facts and effects, i.e.
a
g
ainst a time axis, to identif
yp
recedin
g
causes. The
data can be collected accord
i
n
g
toaf
i
xed
p
la
n
(
ⴝ
p
ro-
l
ective
)
o
r generated before the study beg
i
n
s
(
ⴝ
retro
l
ec
-
t
ive). Furthermore
,
a distinction is made between
f
ollowin
g
the individual course from the time the caus-
a
t
i
ve factor a
pp
ears throu
g
h to the onset of effec
t
(
ⴝ
c
ohort
)
a
nd follow
i
ng the
i
nd
i
v
i
dual course from the
onset of effect back to the earliest possible point in tim
e
when the causative factor a
pp
eare
d
(
ⴝ
t
rohoc
)
(
A.R.
F
e
in
s
tein
,
1977
)
. Thus, a retrospect
i
ve study
i
s deemed
s
cientifically correct if its execution is justified and the
m
ethodolo
gy
is clearl
y
defined. • A
p
ros
p
ect
i
ve stud
y
s
tarts from causat
i
ve factors, observ
i
n
g
the effect ove
r
the course of t
i
me.
(
7, 10, 12)
Sp
ecial case
s
a
r
e the
open
(
non-
bl
in
d)
stu
dy
o
n
the o
n
e
ha
n
da
n
d the
crossover stu
dy
o
n
t
h
eot
h
e
rh
a
n
d.
• Thi
s
means that the controlled cl
i
n
i
cal study
i
s “fundamen
-
tally” (
i
.e. w
i
th some except
i
ons) the sole and mos
t
e
ssential tool for obtainin
gp
roof of the efficac
y
of
a
g
iven substance. If the conditions for a controlled clin-
i
cal study cannot be met, then
i
t must be d
i
spensed w
i
th.
Th
e t
yp
o
l
o
gy
of cl
i
n
i
cal stud
i
es d
i
fferent
i
ates four t
yp
e
s
accord
i
ng to the
i
ra
i
ms:
(
1
.
) pharmacolog
i
cal stud
i
es
,
(
2
(
(
.
)
thera
p
eutic ex
p
lorative studies,
(
3
.)
thera
p
eutic con
-
firmative studies, and
(
4
.)
dru
g
-monitorin
g
studies. Th
e
p
urpose of the last-ment
i
oned group
i
stodef
i
ne the
cost/benef
i
trat
i
o more prec
i
sely,
i
dent
i
fy rare s
i
de
e
ffects and
p
rovide better dosa
g
e recommendations.
2
.
2Pr
ob
l
e
m
so
f
c
l
i
n
ica
l
studies
T
here is a vast arra
y
of literature dealin
g
with still con
-
trovers
i
al aspects of controlled cl
i
n
i
cal stud
i
es.
•
W
e
s
hould be aware that on the one hand
,
medicine is not an
e
xact science an
d
on t
h
eot
h
er
h
an
d
,
h
umans
d
o not re
p
re
-
s
ent a quanti
f
ia
bl
emo
d
e
l
wit
hd
ata on ca
ll
as nee
d
e
d
.
P
roblems
i
ncl
i
n
i
cal stud
i
es often ar
i
se
in
d
i
fferent f
i
elds:
1
. eth
i
ca
l
4
. psycholog
i
ca
l
2
. methodological 5. heuristic
3
.le
g
a
l
6. eco
n
o
m
ic
P
roof
i
n the str
i
ct sense cannot be del
i
vered by a con-
trolled cl
i
n
i
cal study, wh
i
ch has been called the “sacred
co
w”
.
(
5
)
However, the prob
a
bility of statistical error in
a
terms of the chosen tar
g
et criteria can be fixed i
n
advance. In clinical studies, different inter
p
retations o
f
r
esults are st
i
ll poss
i
ble, s
i
nce “
intuitive medical obse
r
va
-
tion and
j
udgement remain indispensable in the individual
Ch
a
p
ter 4
0
c
ase
”
(
E.
B
uc
hb
o
rn
,
1982
)
.
•Th
e
tria
d
of emp
i
r
i
c
i
sm,
i
ntu-
i
t
i
o
n
a
n
d
lo
g
i
c
is necessary in both diagnosis and treat
-
m
e
n
t
(
R.
G
ross, 1988
)
.
2
.
3
Placeb
o
A
placebo (Latin, “I shall please”) or ADT
(
⫽
a
n
ywha
t
yo
u
d
es
ir
e
t
hin
g)
is a “dumm
y
” without an
y
active sub
-
stance,
i
dent
i
cal
i
na
pp
earance to the res
p
ect
i
ve act
i
v
e
d
rug and not des
i
gned to be effect
i
ve. Th
i
s term has
bee
nkn
o
wn
s
in
ce t
h
e
14
th
c
entur
y
.
(
4)
•
In med
i
c
i
ne,
a
placebo assumes two ro
l
es
:
(
1
.) as a therapeut
i
c agent
in
t
he practical treatment of patients, intended to have a
n
“
effect” on a disease or a s
y
m
p
tom, or exertin
g
suc
h
effects without the physician’s knowledge, and (
2
(
(
.
)
as
a
control substance
i
ncl
i
n
i
cal stud
i
es w
i
th drugs. • I
n
i
ndividual cases
,
even objective
c
hanges in physiological
fu
n
ct
i
o
n
sa
n
d
s
p
ec
i
f
ic
eff
ects ma
yb
e
d
emonstra
bl
e. T
h
e
f
orm of adm
i
n
i
strat
i
on and the dosa
g
eofa
p
lacebo, the
phys
i
c
i
an’s personal
i
ty (and that of the pat
i
ent) and th
e
i
ntensity of the disease situation may lead to a weaken
-
i
n
g
or
p
otentiation of the
p
lacebo effect. The im
p
ortant
(i
nd
i
v
i
dual and soc
i
al
)
eth
i
cal
i
ssues assoc
i
ated w
i
th
placebo adm
i
n
i
strat
i
on concern both the pat
i
ent and th
e
physician, who have to be informed in general about
such
p
rocedures. These issues have been clarified b
y
law
a
fter be
i
n
g
d
i
scussed
i
n deta
i
l and assessed on the bas
is
o
f exper
i
mental f
i
nd
i
ngs
.
䉴
The
p
lacebo effect in controlled clinical studie
s
s
hould never be re
g
arded as “zero”, even thou
g
h this
i
s, of course, des
i
red
(
or even
i
m
p
uted
)
from th
e
s
tat
i
st
i
cal v
i
ewpo
i
nt.
Wi
th
i
n the sco
p
eofcl
i
n
i
cal stud
i
es, valuable econom
ic
i
nformat
i
on on med
i
cal procedures can (and should) b
e
obtained. Today
,
eco
n
o
mi
c assess
m
e
n
t
a
ssumes a special
role in clinical studies, and because of its com
p
lex strati-
fi
cat
i
on and the
g
eneral need for rat
i
onal
i
zat
i
on, e.
g
.
i
n
terms of the cost/benef
i
t analys
i
s,
i
t
i
sl
i
kely to become
m
ore and more important. The quality-adjusted lif
e
y
ea
r
(
G. W.
T
o
rr
a
n
ce
,
1987)
s
hould be
i
ncluded
i
nth
e
assessment. (s. p. 878
)
2
.4 Difficult
y
of evaluation
P
rov
i
ng the eff
i
cacy of a (surg
i
cal or med
i
c
i
nal) thera-
p
eut
i
c measur
e
⫺
and this also applies in hepatolog
y
⫺
i
sver
y
difficult, as it mainl
y
de
p
ends on
t
w
o facto
r
s:
1
. non-comparab
i
l
i
ty of
i
nd
i
v
i
dual humans
2. non-com
p
arabilit
y
of individual diseases
S
tatistical methods cannot render eithe
r
non
-
compar
-
a
b
i
l
i
t
y
of individual humans or that of diseases com
p
ar
-
able
⫺
a
t best, the
y
ma
y
com
p
ensate
i
tb
y
means o
f
l
arge pat
i
ent numbers or are able to assess samenes
s
8
7
4
under certa
i
nc
i
rcumstances.
(
1, 5
)
•S
tat
i
st
i
ca
l
compar
-
a
bility
o
f different patient groups can only be achieved
if
t
hree re
q
u
i
rements
a
r
e
m
et:
1. e
q
ual
i
t
y
of structure
2. equal
i
ty of observat
i
on
3. equality of representation
E
ven with
g
reat dia
g
nostic effort, no convincin
g
s
truc-
t
ura
l
equa
l
ity
i
s obtainable. Conse
q
uentl
y
, randomiza-
ti
on alone does not guarantee a valuable cl
i
n
i
cal study.
Desp
i
te these problems
,
t
hree study types
s
hould (and
must
)b
e use
d:
1
.
E
x
a
min
at
i
o
n
o
f
e
ff
ect
⫽
chan
g
einan
y
one
p
aramete
r
2.
E
xamination of efficacy
⫽
cureorim
p
rovement of diseas
e
3.
E
xamination of superiorit
y
⫽
im
p
rovement of
p
arameters, or cure, o
r
i
m
p
rovement of disease b
y
conventional
th
era
py
vs. new t
h
era
py
2.5 Provability of treatmen
t
I
ncl
i
n
i
cal stud
i
es
i
nvolv
i
ng drug
s
⫺
this also applies t
o
h
epato
l
og
y
⫺
t
he terms “effect” and “efficac
y
”havenot
alwa
y
s been a
pp
ro
p
riatel
y
distin
g
uished, but were often
(
erroneously) cons
i
dered
i
dent
i
cal. • Th
e
e
ffect of a spe
-
c
i
f
i
c drug (or “l
i
ver therapeut
i
c”) show
i
ng changes
i
n
an
y
measured
p
arameters or reactions is easier to
p
rove
t
han its efficac
y
in the sense of cure or im
p
rovement of
d
i
sease. Therapeut
i
c eff
i
cacy
(
or eff
i
cacy of “l
i
ver ther-
apy”)
i
s def
i
ned by the d
i
fference between the un
i
nflu
-
e
nced disease course
(
i.e.
p
ossible or usual course
)
and
t
he disease course chan
g
ed b
y
thera
p
eutic measures
(
i.e
.
actual course)
.
There is, however, no chance of ever
o
bserving and assessing the “possible” and the “actual”
d
isease course simu
l
taneous
ly
.
(
1
.
)Th
e
m
arketability of a pharmaceut
i
cal preparat
i
o
n
is controlled by an act of administration. In this context,
t
hr
ee c
r
ite
r
ia
m
ust be satisfied for the licensin
g
of medic-
aments,
i
nclud
i
n
g
“l
i
ver thera
p
eut
i
cs”
:
1.
qua
l
it
y
2
. sa
f
ety
3
.
e
fficac
y
(
2
(
(
.
)
T
h
eterm“
q
ual
i
t
y”
is defined b
y
various criteria:
p
urit
y,
i
dent
i
t
y
, content,
g
alen
i
c
p
ro
p
ert
i
es and tem
p
erature sta-
bi
l
i
ty of a substance. • The ter
m
“sa
f
ety
”
i
s def
i
ned
i
n
r
elation to acute and chronic toxicit
y
, foetal toxicit
y
and
fertilit
y
,muta
g
enic and carcino
g
enic
p
otential.
(
3
.
) As regards the term
“
efficacy”
,
no legal definition
e
xists. As a rule, efficac
y
is defined b
y
the sum of desired
Treatment o
fl
iver
d
isease
s
e
ffects w
i
th regard to a certa
i
n therapeut
i
ca
i
m. Thus
,
i
n terms of the licensing regulations, the efficacy of a
dru
g
, includin
g
“liver thera
p
eutics”, ma
y
be defined a
s
“
t
h
ea
b
stract qua
l
ity o
f
me
d
icine to ac
h
ieve t
h
erapeuti
c
success with proper use, accidental and placebo success
h
avin
g
been excluded
”
(
K.J.
H
ennin
g
,
1978
)
.
T
h
eUSFoo
d
,
D
rug and Cosmet
i
c Act def
i
nes the term “eff
i
cacy”
i
n
a
s
imilar manner. • Mere proof of quality and safety i
s
s
ufficient for medicine that does not have be licensed
,
but onl
y
re
gi
stered; no
p
roof of eff
i
cac
yi
sre
q
u
i
red. Th
is
a
ppl
i
es to homoeopath
i
c remed
i
es, for example.
(
4
.) The eff
i
cacy of med
i
c
i
nal remed
i
es,
i
nclud
i
ng “l
i
ve
r
therapeutics”, may be regarded as a
c
ontinuum, i
.e.
fr
om
“
ver
y
wea
k”
to
“h
ig
hly
potent
”
.
T
hus, efficac
y
is also
p
roven when the substance
i
s shown to be onl
y
sl
ig
htl
y
effect
i
ve or
i
s only effect
i
ve
i
n some pat
i
ents (
i
nd
i
v
i
dual
c
ases). Principally (
⫽
e
xceptions are possible), proof o
f
efficac
y
is to be
p
rovided b
y
controlled clinical studies
.
No
p
roof of su
p
er
i
or
i
t
y
of the dru
g
under
i
nvest
ig
at
i
o
n
over the standard preparat
i
on
i
s requ
i
redbylaw.No
r
d
oes the licensing procedure check whether there is
a
p
otential need for the dru
g
in
q
uestion
.
T
hus the aim of clinical studies is to provide proof o
f
sa
f
et
y
and a
pp
ro
p
riate e
ff
icac
y
. • However, it is essen-
ti
a
l
to ensure t
h
e
q
ua
li
t
y
o
f
t
h
eran
d
om
i
ze
d
, contro
ll
e
d
t
rials in every respect
!
(9
)
3
Principles of liver therap
y
3.1 Bas
i
c cons
i
derat
i
ons
First of all, two terms need rectif
y
in
g
, since th
e
su
p
erficial
y
et incorrect use of the desi
g
nation
s
“live
r
t
herapy” an
d
“
protective therapy of the liver
”
have
rendered
i
t fundamentally more d
i
ff
i
cult to make
accu
r
ate state
m
e
n
ts.
Th
ese te
rm
sa
r
e
r
e
li
cs
fr
o
m
t
h
e
e
p
ochs of s
p
eculative or em
p
irical thera
py
and con
-
s
t
i
tute the or
i
g
i
n of the catchword “therapeut
i
cn
i
h
i
l-
i
sm”. (s. tab. 40.1)
3.1.1 L
i
ver thera
py
T
here has never been and there st
i
ll
i
s not any “l
i
ve
r
thera
py
” in the true sense ⫺
a
nd no such thera
py
will
exist in future either. The liver as the lar
g
est biochemica
l
p
erformance centre of the bod
yi
s constantl
y
act
i
ve
in
s
ome 11 ma
j
or metabol
i
c areas w
i
th 60
⫺
7
0
i
ntegrated
p
artial functions. In order to accom
p
lish the man
y
tasks, about 300 billion liver cells undertake a
pp
rox. 50
0
b
i
omolecular react
i
ons da
i
l
y
⫺
i
ndeed an unbel
i
evable
f
eat. Consequently,
i
t
i
s not poss
i
ble for drugs to have
a
n
e
ff
ect o
n
t
h
e
liv
e
r
as a
wh
o
l
e.
However
,
rr
t
hera
p
ies fo
r
l
i
v
e
r
diseases
o
rt
h
erapies
f
or
h
epato
l
ogica
l
symptoms are
available.
W
i
th th
i
sl
i
ngu
i
st
i
c correctness, our therapeu-
8
75
t
i
c efforts
i
n hepatology become
r
ealistic
a
nd objectifi
-
able
.
There are far more than 100 liver diseases plus
v
ariants and diverse com
p
lications. A lar
g
e number of
t
hem can be treated successfull
y
w
i
th
p
harmacolo
gi
cal
r
eg
i
men
s
⫺
somet
i
mes w
i
th str
i
k
i
ngly good result
s
⫺
as
w
ell as, of course, by invasive and surgical therapy
.
3
.1.2 L
i
ver thera
p
eut
i
ca
g
ents
I
n the str
i
ct l
i
ngu
i
st
i
c and hepatolog
i
cal sense, there
is
n
o such thing as liver therapeutic agents. How
e
v
er,
t
hi
s
u
n
f
ortunate ter
m
i
sfre
q
uentl
y
⫺
and indeed deliberatel
y
⫺
used rhetor
i
call
yi
n
p
ubl
i
cat
i
ons or for adm
i
n
i
strat
i
v
e
r
easons. Here, the express
i
o
n
“hepatic agents”
(
analo-
gous to cardiac, otologic and diuretic agents, etc.) woul
d
b
e more correct and not so
p
romisin
g
in the
p
o
p
ular
sense as the des
ig
nat
i
on “l
i
ver thera
p
eut
i
ca
g
ents”. •
In
any case, one ought to be aware of the possible psycholog
-
ical e
ff
ect o
f
such a term, especiall
y
with regard to
a
“pl
ace
b
o
”
.
(
s.
p
. 874
)
3
.1.3 Protect
i
ve thera
py
of the l
i
ve
r
S
imilarly, there is no generally protective therapy of the
liver. Liver “
p
rotection” as such ma
y
include active
v
acc
i
nat
i
on a
g
a
i
nst v
i
ral he
p
at
i
t
i
s A or B, for exam
p
le
,
and,
i
naw
i
der sense, also pass
i
ve
i
mmun
i
zat
i
on after
e
xposure or general avoidance of typical liver noxae
.
This can “
p
rotect” the liver from diseases
.
(16
)
I
n
i
n-v
i
tro
a
n
d
i
n-v
i
vo ex
p
er
i
ments
,
certa
i
n substance
s
can be stud
i
ed for the
i
r protect
i
ve effect on the hepato-
c
y
tes or endothelial cells
(
includin
g
biomembranes an
d
or
g
anelles
)
under the influence of various noxae or
tox
i
ns. Many su
b
stances
h
ave
b
een s
h
own to
d
isp
l
ay
d
is
-
tinct protective properties experimentall
y
under various
i
nvesti
g
ative con
d
itions.
S
uch studies are not
,
h
o
w
e
v
er,
admissible in humans. • These ex
p
erimental
p
rotectiv
e
p
ropert
i
es may also be of therapeut
i
c value
i
n
i
nd
i
v
i
dual
cases (e.g. appl
i
cat
i
on o
f
s
ilibini
n
i
n Aman
i
ta po
i
son
i
ng)
.
A“l
i
ver-protect
i
ve preparat
i
on” must therefore be cap
-
able of
p
rotectin
g
the he
p
atoc
y
tes
(
as well as the sinu
s
e
ndothelium
)
from a
p
articular liver toxin, or from tw
o
to three clearly def
i
ned (or,
i
n the opt
i
mal case, all obl
i-
gate) l
i
ver tox
i
ns
,
b
y
administration be
f
ore or, at the lat
-
e
st, w
h
en t
h
e
d
ama
g
e occurs. Th
e use o
f
a substa
n
ce
i
n
e
xistin
g
cellular dama
g
e would be classified as “ther-
apy” and no longer “protect
i
on”. The term protect
i
ve
l
i
ver therapy clearly
i
mpl
i
es prophylax
is
⫺
w
h
i
ch, apar
t
from the above exce
p
tions
(
e.
g
. vaccination
)
, is usuall
y
n
ot feasible under the
p
rovisions of the res
p
ective health
i
nsurance system.
(16
)
3.2 Precond
i
t
i
ons
T
he
q
uestion of
p
rovabilit
y
of a certain thera
py
is als
o
de
p
endent on various
facto
r
s
in he
p
atolo
gy
:
(
1
.) k
now-
ledge of the spontaneous course of a l
i
ver d
i
sease (not
Ch
a
p
ter 4
0
known
i
n
i
nd
i
v
i
dual cases, but only globally assessable)
,
(
2
(
(
.
) endogenous factors (gender, age, genetics), and (
3
.)
exo
g
enous influence
(
e.
g
. lifest
y
le, noxae,
p
atient com
-
p
l
i
ance
)
. These
i
m
p
onderables can scarcel
y(i
f at all
)
be
i
ntegrat
i
vely assessed or excluded even us
i
ng subtle stat-
ist
i
ca
lm
et
h
ods.
R
a
n
do
miz
at
i
o
n
a
n
d doub
l
e
-
b
lin
dc
lin-
ica
l
t
ri
a
l
sca
n
do
n
o
m
o
r
et
h
a
n
ba
l
a
n
ce out t
h
ese d
iff
e
r
-
ences. In order to obta
i
n usable data, certa
in
s
tat
i
st
i
cal
c
ondition
s
s
hould be fulf
i
lled as far as poss
i
ble:
⫺
homogeneous f
i
nd
i
ngs
in
⫺
homo
g
eneous
p
atient
s
with
⫺
homogeneous d
i
seas
e
T
hese re
q
u
i
rements are d
i
ff
i
cult to meet even
i
n con
-
trolled cl
i
n
i
cal stud
i
es
i
n hepatology. Moreover, the us
e
o
fm
ed
i
cat
i
o
ninliv
e
r
d
i
sease
i
s based o
nf
u
r
t
h
e
r
esse
n-
t
i
a
l
c
l
i
n
ica
l
co
n
ditio
n
s:
1
. Deta
i
led hepat
i
cd
i
agnos
i
sw
i
th exact class
i
f
i
cat
i
on
o
f
t
h
e
liv
e
r
d
i
sease
2
.
I
de
n
t
ifi
cat
i
o
n
a
n
de
limin
at
i
o
n
o
f
t
h
e causat
iv
e
noxa
(
e
)
3
.El
i
m
i
nat
i
on of concom
i
tant negat
i
ve factors or
add
i
t
i
o
n
a
ln
o
x
ae
T
herapeut
i
c uncerta
i
nt
i
es or d
i
ffer
i
ng conclus
i
ons re-
g
ard
i
ng drug effects or eff
i
cacy may thus be attr
i
bute
d
to var
y
in
g
de
g
rees of methodolo
g
ical inaccurac
y
:
⫺
di
fferent d
i
sease courses
with
⫺
d
ifferent
p
atho
g
enesi
s
in
⫺
di
fferent pat
i
ent
s
and an
⫺
i
nsufficient detailed dia
g
nosi
s
were subm
i
tte
d
to
⫺
j
oint statistical evaluation
3
.3 Formsof“l
i
ver therapy”
C
ausal treatment of l
i
ver d
i
seases, wh
i
ch
i
s rarely (
i
f
ever
)
feasible, should achieve the com
p
lete eliminatio
n
of the actual cause
(
s
)(
e.
g
. elimination of the causativ
e
noxa, ant
i
v
i
ral treatment, gene therapy
i
n hered
i
tary
li
ver d
i
seases).
•
T
reatment of pathogenetic primary reac
-
t
i
o
n
s
(
e.
g
. with interferon, immunosu
pp
ressants or
p
eni
-
c
illamine
)
is aimed at interru
p
tin
g
the “
p
ostcausal
”
p
athogenes
i
s.
•
Treatment of d
i
sease progress
i
o
n
i
nter-
v
enes
i
n the patholog
i
cal process
i
n a last
i
ng and eff
i-
c
ient manner and thus
p
revents or slows down the
g
en
-
erall
y
dan
g
erous conse
q
uences
(
e.
g
. inhibition of
c
holestas
i
s, f
i
brogenes
i
s and portal hypertens
i
on).
•
8
76
A
lmost all substances used
i
n hepatology are classe
d
as
s
ymptomatic treatment
.
These substances help (
1
.) to
combat malaise and disturbances secondar
y
to the live
r
disease (e. g. antipruritics), and (
2
(
(
.
)
to
i
nfluence th
e
structures and funct
i
ons of the hepatocytes and endo
-
t
helial cells as well as the bile capillaries (e.g. antioxi
-
dants, essential
p
hos
p
holi
p
ids, UDCA, sil
y
marin
).
(16
)
3
.
4 Aim
so
f
t
r
eat
m
e
n
t
Drug therapy of a part
i
cular l
i
ver d
i
sease or compl
i
ca-
ti
ve development must have bas
ic
t
reatment aims
.
T
h
e
p
rimar
y
thera
p
eutic aim is to eliminate the existin
g
causative factors and
p
atho
g
enetic mechanisms. Th
e
f
i
nal goal
i
salwaysthe
rehabilitation
o
f the l
i
ver pat
i
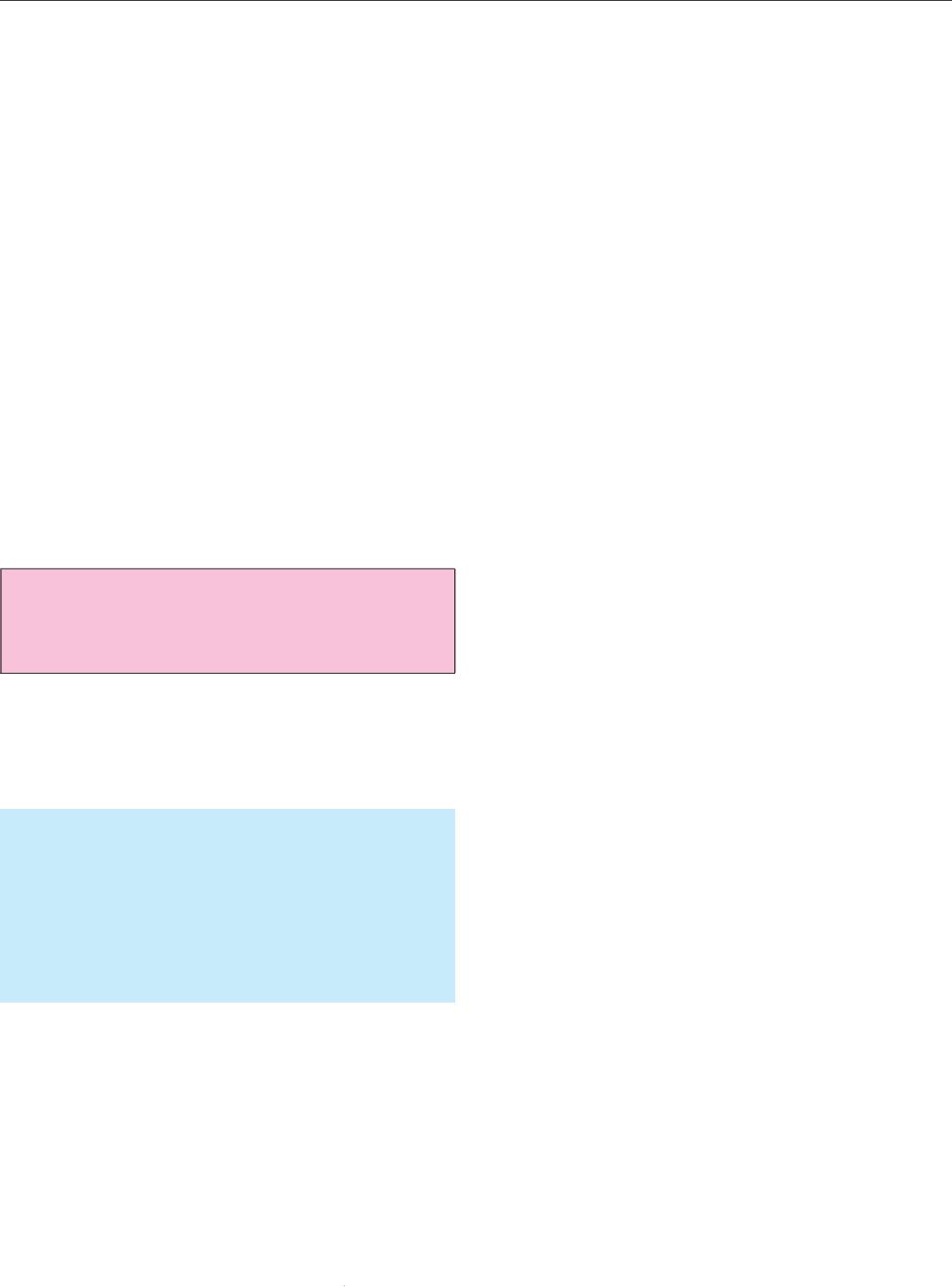
ent.
(
s. tab. 40.2) (s. p. 912
)
1. Eliminatin
g
or definitivel
y
overcomin
g
the caus
e
of disease
(
as far as
p
ossible
)
as well as
p
romotin
g
and s
p
eed
i
n
g
u
pi
ts cur
e
2. Inhibition of inflammator
y
reactions
3. Curbin
g
of mesench
y
mal reactions
4
. Modulat
i
on of
i
mmunolog
i
cal react
i
on
s
5
. Support/normal
i
zat
i
on of l
i
ver cell funct
i
on
s
6. Stimulation of hepatic regeneration
Rehab
i
l
i
tat
i
o
n
Ta
b
.
4
0.
2
:
T
reatment a
i
ms
i
nl
i
ver d
i
sease
s
䉲
䉲
䉲
䉲
䉲
䉲
3.5
C
ategor
i
es of “l
i
ver therapeut
i
cs
”
A
number of substances and
p
re
p
arations are availabl
e
for the treatment of liver diseases. The
y
can be cate
g
or
-
i
zed
i
nvar
i
ous ways. (s. tab. 40.3
)
1
.
P
ro
p
h
y
lactics: e.
g
. immuno
g
lobulins or vaccines
a
g
ainst he
p
atotro
p
ic virus infections
2
.
Ant
i
dotes: e.g. s
i
l
i
b
i
n
i
naga
i
nst Aman
i
t
a
p
o
i
son
i
ng or N-acetylcyste
i
ne
i
n paracetamo
l
intoxication, haemar
g
inate in acute
p
or
p
h
y
ri
a
3
.
P
r
i
mar
y
l
i
ver thera
p
eut
i
cs
:
e
.
g
.
p
enicillamine,
glucocort
i
co
i
ds, azath
i
opr
i
ne,
i
nterferon-
α
,
a
i
med
at pr
i
mary
i
ntervent
i
on
i
n the aet
i
ology o
r
p
athomechanism of liver disease
.
4.
S
econdar
y
l
i
ver thera
p
eut
i
cs:
e
.
g
.
f
at-so
l
u
bl
e
vi
tam
i
ns
i
n
i
mpend
i
ng def
i
c
i
ency states, drugs t
o
reduce portal hypertens
i
on, substances to rel
i
eve
h
yp
erammoniaemia, aimed at secondar
yp
reven-
t
ion of the various se
q
uelae of liver disease
.
Tab. 40.3:
C
ategories of liver therapeutic agent
s
3.6 Act
i
ve substance
s
F
or several
y
ears,
(
ne
g
ative
)
claims a
pp
eared in the
p
res
s
stat
i
n
g
that the
p
harmaceut
i
cal market was over
-
Treatment o
fl
iver
d
isease
s
saturated w
i
th more than 600 l
i
ver preparat
i
ons
.
A
lthough the originator of this claim was not identified
,
t
his uto
p
ian number made the rounds. • In fact, there
are mere
ly
2
5 substances or
g
rou
p
s of substance
s
(
o
f
chem
i
cal or plant or
i
g
i
n) l
i
sted
i
n the pharmacopoe
i
a.
Here, the various preparations containing the same sub-
stance are numbered se
p
aratel
y
, which
g
ives a total o
f
90
ⴚ
100 l
i
sted
p
re
p
arat
i
on
s
.
•It
i
s
i
rres
p
ons
i
ble tha
t
some “l
i
ver therapeut
i
cs” st
i
ll have an a
l
co
h
o
l
conten
t
of
2
5
⫺
66 vol.% (particularly homoeopathic and phyto
-
t
hera
p
eutic remedies
)
.
(
s.
p
.64
)
Althou
g
h the ofte
n
q
uant
i
tat
i
vel
y
low
i
ntake of alcohol
i
na
p
re
p
arat
i
o
n
may be “harmless” (even “3 t
i
mes da
i
ly”),
i
tw
i
ll usually
cause a relapse in an abstinent alcoholic
.
In principle
,
th
ereisno
j
usti
f
ia
bl
e argument
f
or
k
eeping t
h
ea
l
co
h
o
l
content in a
h
e
p
ato
l
ogica
lp
re
p
aration
!
Some dru
g
s with
sp
ecial indications
a
r
e used
in liv
e
r
d
i
s-
e
ases or in certain com
p
lications. The
y
are not found in
t
he s
p
ec
i
al cate
g
or
y
of l
i
ver thera
p
eut
i
cs
(p
harmaco-
poe
i
a), but are l
i
sted accord
i
ng to the
i
rma
i
n
i
nd
i
cat
i
on.
Treatment with some of these active substances ma
y
be
accom
p
anied b
y
side effects.
(
s. tab. 40.4
)
C
hem
i
cal substances (or
g
rou
p
s)
1
.
AA
o
f
t
h
eureac
y
c
l
e
2. Beta blockers
3.
Bil
eac
i
ds
4
.BC
AA
5. Deferoxam
i
ne
6. D-pen
i
c
i
llam
i
n
e
7.
Di
u
r
et
i
cs
8
. Glucocorticoids
9. Haemar
gi
nate
10. Immunosuppressants
11
.
Imm
u
n
ost
im
u
l
a
n
ts
12
.
L
actulose
13. Nucleos
i
de analogue
s
14. S-adenosyl-L-meth
i
on
i
n
e
15.
S
omatostati
n
16. S
p
ironolacton
e
17. V
i
rustat
i
c
s
18. V
i
tam
i
ns (
A
⫺
K
)
19
.
Zin
c
Ph
y
tothera
p
eut
i
ca
g
ents (or
g
rou
p
s
)
1. Colch
i
c
i
n
e
2. Essent
i
al phosphol
i
p
i
d
s
3. Gl
y
c
y
rrhizi
n
4
. Sil
y
marin
5
.Var
i
ous herbal preparat
i
on
s
Ta
b
.
4
0.
4
: Act
i
ve chem
i
cal substances (or groups) and phytothera-
p
eut
i
ca
g
ents used
i
n some l
i
ver d
i
seases or the
i
r com
p
l
i
cat
i
ons
Acti
v
e substa
n
ces
w
ith
p
roven efficac
y
in he
p
atolo
gy
a
r
e
o
n
l
ya
d
ministere
d
as
“
treatment
”
an
d
not as
“l
iver protec-
8
77
tion” (apart from the prophylactics mentioned above
)
.
T
hese active substances are used in patients when,
accordin
g
to the dia
g
nosed disease and the clinical an
d
p
harmacolo
gi
cal results, the
y
are actuall
yi
nd
i
cated.
•
Thus, it is the existing liver disease and/or complication
and not the medication budg et or the patient’ s wishes whic
h
d
eci
d
es t
h
et
h
era
p
eutic in
d
ication.
•
An
y
thin
g
else would
g
oa
g
a
i
nst the
p
r
i
nc
ip
les of a
p
h
y
s
i
c
i
an or be uneconom-
i
cal, and legally problemat
i
c
i
n
i
nd
i
v
i
dual cases
.
T
he second d
i
mens
i
on of controlled stud
i
es
,
“t
i
me”
,
is
frequently g
i
ven
i
nsuff
i
c
i
ent cons
i
derat
i
on
i
n evaluat
i
n
g
therapeutic results. In fact, it is only possible to asses
s
w
h
et
h
e
r
t
h
e substa
n
ces used
in
c
hr
o
ni
c
liv
e
r
d
i
sease
h
ave the re
q
u
i
red eff
i
cac
y
after an ade
q
uate treatmen
t
p
er
i
od. In the drug therapy of pat
i
ents w
i
th chron
i
cl
i
ver
disease as carried out by the clinician and general prac-
titioner, evaluation
p
eriods invariabl
y
extend over sev
-
e
ral
y
ears. In such cases,
p
os
i
t
i
ve or ne
g
at
i
ve results can
be obta
i
ned “emp
i
r
i
cally”, but because they are not
“statistically” confirmed, they are not “provable”. I
n
this context as well,
•
emp
i
r
i
c
i
s
m
•
i
ntu
i
t
i
o
n
•
l
o
g
ic
ma
y
diver
g
e
(
s.
p
. 873
)
, so that statistics, which as such
are
i
nd
i
spensable, may
i
ndeed prove to be an obstacle.
P
erhaps the expectat
i
ons or requ
i
rements of “l
i
ver ther
-
apy” are too h
i
gh. W
i
th regard to other organs and the
ir
r
es
p
ective diseases, established medication often does no
t
r
eall
y
achieve a “cure”, but merel
y
“functional im
p
rove-
ments” (e.g. recompensat
i
on,
i
nh
i
b
i
t
i
on of progress
i
on
,
s
tab
i
l
i
zat
i
on
in
everyday l
i
fe
,
i
mprovement
i
n qual
i
ty of l
i
fe,
r
ehabilitation
)
.In
p
rinci
p
le, these full
y
acce
p
table thera
py
aims a
pp
l
y
to the treatment of liv
e
r
d
i
s
eases as
w
ell.
3.7 Dose ad
j
ustment of med
i
cament
s
L
iv
e
r
a
n
d
m
ed
i
ca
m
e
n
ts a
r
e
in
te
rr
e
l
ated
in
t
hree wa
y
s
:
1. Med
i
cat
i
o
n
inducing
li
ver d
i
seases
2.
M
ed
i
cat
i
on
for
l
iv
e
r
d
i
seases
3.
M
ed
i
cat
i
on
changed by
l
iv
e
r
d
i
seases
Apart from the k
i
dneys, the l
i
ver
i
s the most
i
mportan
t
excretory organ for drugs. In contrast to other mech
-
a
nisms of dru
g
elimination, which are relativel
y
wel
l
u
n
d
erstoo
d
,
li
ver metabol
i
s
m
o
fd
ru
g
s
h
as
p
rove
d
extremely compl
i
cated. (s. pp 5
6
⫺
60)
B
iotransformation
is influenced by variable and non-variable factors unde
r
p
h
y
siolo
g
ical and
p
atholo
g
ical conditions.
(
s. tab. 3.18
)
•
C
han
g
es
i
n
p
harmaceut
i
cal
p
re
p
arat
i
on
s
are alterat
i
on
s
i
n the respect
i
ve propert
i
es wh
i
ch occur due to the d
i
s
-
turbed metabolization function of the liver cells and
/
o
r
he
p
atic blood flow secondar
y
to liver disease. Addition
-
a
ll
y
, dru
g
metabol
i
sm ma
y
be drast
i
call
y
mod
i
f
i
ed b
y
Ch
a
p
ter 4
0
c
oex
i
st
i
ng hypoalbum
i
naem
i
a or cholestas
i
s. L
i
ver d
i
s
-
eases do not only affect the elimination parameters (e.g
.
half-life, clearance
)
, but also absor
p
tion
(
e.
g
. bioavail
-
a
b
i
l
i
t
y)
and d
i
str
i
but
i
on of the dru
gi
n the bod
y
. A fur-
ther factor are the
i
nteract
i
ons of certa
i
n drugs w
i
t
h
receptors at the site of action (e.g. increased sensitivit
y
of the brain to diaze
p
am in cirrhosis
p
atients
)
. Biotoxo
-
m
etabol
i
tes and l
ipi
d
p
erox
i
dat
i
on, wh
i
ch are not nor-
m
ally typ
i
cal of a certa
i
n med
i
cament, must also be
a
nticipated. • In principle, a
dose
r
educt
i
o
n
s
h
ou
l
dbe
c
onsidered in severe and chronic liver disease, es
p
eciall
y
when the med
i
cament
i
s used re
g
ularl
y
. On the other
hand
,a
d
ose increase may be requ
i
red
i
n
i
.v. adm
i
n
i
stra-
tion owing to reduced hepatic blood flow and usin
g
m
edication with a hi
g
h elimination rate. • Disturbe
d
d
ru
g
metabol
i
sm ma
y
be further a
gg
ravated b
y
alcohol
c
onsumpt
i
on w
i
th
i
ts mult
i
ple b
i
ochem
i
cal effects. (s. p
.
6
5) (s. tabs. 28.2, 28.3)
D
es
p
ite
g
reat efforts, it has not been
p
ossible so far t
o
m
ake s
i
ngle dose calculat
i
ons
(
1
.) for a
ce
r
tain
m
ed
i
ca
-
ment, (
2
(
(
.)
i
nacerta
i
n l
i
ver d
i
sease, and
(
3
.
)
i
n
a
c
erta
in
p
atient. Some dru
g
s have been classified into thre
e
g
rou
p
s on the basis of their he
p
atic extraction rate and
route as well as the
i
r form of adm
i
n
i
strat
i
on: drugs w
i
th
a
h
i
gh, w
i
th a moderate and w
i
th a low r
i
sk of overdos
-
age
⫺
h
owever
,
s
uch information is
g
iven with reserva
-
tions. The difficulties re
g
ardin
g
the correct dose ad
j
ust-
m
ent of a med
i
c
i
nal remedy
i
n therapeut
i
c use requ
i
r
e
c
arefu
l
monitorin
g
of the
i
nd
i
v
i
dual pat
i
ent, somet
i
mes
a
lso determination of the blood values
,
or consultation
with a
p
harmacolo
g
ist.
(
16
)
䉴
C
lini
ca
l
stud
i
es:
I
nvi
e
w
o
f
t
h
eabo
v
e
-m
e
n
t
i
o
n
ed
d
ifficulties, it ma
y
be
p
roblematic to administer the
same
d
ose to
all
v
olunteers and to obta
i
n pharmaco
-
l
og
i
call
y
e
quivalent
r
esults
i
ncl
i
n
i
cal stud
i
es. • Th
is
m
i
g
ht also ex
p
lain the occasionall
yg
reat variation i
n
s
tud
y
results
(
des
p
ite a carefull
y
chosen trial desi
g
n
)
a
nd any potent
i
al “
i
neff
i
cacy” or undes
i
red effect o
f
the drug. (s. pp 60, 873, 878
)
3
.8 Si
g
nificance of
q
ualit
y
of lif
e
Of the two d
i
mens
i
ons of l
i
fe, quant
i
ty and qual
i
ty, cl
i
n
-
i
cal studies have inevitably paid far more attention t
o
the former
(
i.e. len
g
th of life
)
.Th
e
q
uant
i
t
y
of l
i
fe
(j
ud
g
ed b
y
surv
i
val
p
robab
i
l
i
t
y
, mortal
i
t
y
rate or sur
-
v
i
val curves) seems to be the most
i
mportant parameter
f
or assessin
g
treatment efficac
y
.Areviewof99
p
ublica
-
tions which a
pp
eared in leadin
g
sur
g
ical
j
ournals fro
m
1981
⫺
1986 revealed that
i
n 97% of the
p
a
p
ers, no men
-
t
i
on was made of qual
i
ty of l
i
fe after surg
i
cal procedures
⫺
in 341
p
ublications on cardiac sur
g
er
y
, this was men-
tioned in onl
y
8% of case
s
(
J. O
’Y
oung
e
ta
l
., 1985, 1987
)
.
Obviousl
y
, the
p
rolon
g
ation of life was
p
aramount i
n
f
i
x
i
ng therapeut
i
ca
i
ms.
(1, 13, 14, 18, 19
)
8
7
8
Def
i
n
i
ng and measur
i
ng th
e
q
uality of lif
e
has becom
e
important in recent years. This also applies to the con-
servative or invasive treatment of liver disease, and, i
n
future, more attent
i
on w
i
ll have to be
p
a
i
dtocr
i
ter
i
a
for assess
i
ng the changed qual
i
ty of l
i
fe under certa
i
n
t
herapies as well as the choice of certain treatment stra-
t
e
g
ie
s
(
M. L
u
d
w
i
g
,
1988).•T
he
d
e
f
initio
n
o
f good l
i
f
e
qual
i
ty
i
mpl
i
es that (
1
.) a person exper
i
ences the leas
t
p
ossible im
p
airment and handica
p
under a
g
iven ther-
apy (
⫽
clinical no
r
m
), (
2
(
(
.
)
this
p
erson functions i
n
a
ccordance w
i
th ex
i
st
i
ng soc
i
al roles and der
i
ves sat
i
s-
f
act
i
on from th
i
s(
⫽
s
ocial nor
m
), and
(
3
.
) the hopes
a
nd ex
p
ectations of this
p
erson are fulfilled
(
⫽
indivi-
dual no
r
m
)
(M. B
u
llin
g
e
r
, 1988)
rr
. • In one com
p
rehens
i
v
e
survey of the l
i
terature, not one s
i
ngle study focus
i
ng on
t
he quality of life in liver disease is cited. • Remarkably
,
a later stud
y
mentioned a si
g
nificant reduction in th
e
q
ual
i
t
y
of l
i
fe
in
p
atients wit
h
c
h
ronic
h
e
p
atitis C.
(
14
)
In
a further stud
y
, interferon treatment was not onl
y
shown
t
o
i
m
p
rove the d
i
sease, but also to enable the
p
at
i
ent
s
t
o resume the
i
r normal da
i
ly rout
i
ne
.
3.9 Assessment of surv
i
val rat
e
I
n
t
h
et
r
eat
m
e
n
to
fliv
e
r
d
i
seases
whi
c
hh
a
v
ea
f
u
lmin
a
n
t
course or which are chronicall
yp
ro
g
ressive
(
and the
r
es
p
ect
i
ve com
p
l
i
cat
i
ons
)
,the
q
uest
i
on of surv
i
val ar
i
ses
.
I
nth
i
s context, the class
i
f
i
cat
i
on accord
i
ng t
o
C
hild
-
T
urcotte (1964) an
d
P
u
g
h (1973) has proved its wort
h
w
orldwide.
(
s. fi
g
. 35.7
)
• We have used this classificatio
n
o
nare
g
ular bas
i
s.
I
n 2000 a score was published giving a prediction of the
survival chances in
p
atients with TIPS.
(
16
)
Sub-
se
q
uentl
y
,th
i
s score was val
i
dated
i
n several cohorts of
pat
i
ents suffer
i
ng from d
i
fferent forms of l
i
ver d
i
seas
e
w
ith varying degrees of severity. The studies included
in
p
atients and out
p
atients in man
y
different
g
eo
g
ra
p
hi-
cal re
gi
ons. The new model was
i
n
i
t
i
all
y
termed “Ma
y
o
e
nd-stage l
i
ver d
i
sease” (MELD). Th
i
s name wa
s
later changed into “Model for end-stage liver disease
”
(
MELD
)
,
althou
g
h the acron
y
m MELD remained
una
l
tere
d.
(
18
)
MELD is based on values relatin
g
to cre-
atinine, bilirubin and INR
(
international normalized
rat
i
o). These values are
i
ncluded
i
n the or
i
g
i
nal mathe
-
mat
i
cal formula for MELD
:
9
.57xlog
c
(creat
i
n
i
ne
)
⫹
3
.78xlo
g
c
(b
i
l
i
rub
i
n)
⫹
11.2 x lo
g
c
(
INR)
⫹
6.
43
⫽
……
4 Nutritional therap
y
o
f
liv
e
r
d
i
seases
The Hi
pp
ocratic idea tha
t
“dy
scrasia
”
was the cause of
nearl
y
all diseases meant tha
t
dietetics
(
⫽
d
iaita
)
was
necessary for th
e
“
restoration to normal of the life order
”
.
Treatment o
fl
iver
d
isease
s
(
s. p. 6) Even
i
n ant
i
qu
i
ty, spec
i
al forms of nutr
i
t
i
o
n
w
ere of great importance in the treatment of liver dis
-
e
ases. In addition to those dietar
yp
rescri
p
tions which
w
ere w
i
th
i
n the reach of ever
y
one
(
e.
g
. donke
y
l
i
ve
r
wi
th parsley and honey) (s. pp 7, 872), there were also
e
xtremely complicated diets for the treatment o
f
j
aundice which onl
y
“kin
g
s” could afford
(
C
e
l
sus
called
j
aund
i
ce th
e
morbus regius
)
. (s. p. 7) • Dur
i
n
g
all historical epochs of medicine, dietetic measures
have
p
la
y
ed an essential role in the treatment of live
r
d
i
sease
s
⫺
e
ven
i
n the so-called “d
i
rt
yp
harmac
y
”o
f
med
i
aeval t
i
mes. (s. p. 872) Because d
i
etet
i
cs assume
d
such an important role in hepatology, nutrition, i. e
.
e
nteral intake of s
p
ecial bevera
g
es and food, was mainl
y
b
ased on m
y
tholo
gi
cal and, at a later date, also on s
p
ec
-
ulat
i
ve
i
deas
.
F
rom the beg
i
nn
i
ng of the 2
0
th
cen
t
ury,
a
mild liver die
t
was
p
ro
p
a
g
ated, which in some cases was
p
ursued with
s
cientific meticulousness. The
p
urists issued strict nutri-
t
i
onal rules for pat
i
ents concern
i
ng l
i
ver d
i
ets. In thos
e
d
ays, we young cl
i
n
i
c
i
ans often had great d
i
ff
i
culty
in
im
p
lementin
g
such
g
uidelines in
p
ractical terms. • This
one extreme was set a
g
ainst the other extreme of thera
-
p
eut
i
cn
i
h
i
l
i
sm,
i
.e.
a
free cho
i
ce of food by the pat
i
ent
(“eat what you l
i
ke”). (s. tab. 40.1)
䉴
N
eit
h
er extreme is acce
p
ta
ble
⫺ in
f
act, certain
l
ive
r
d
iseases or com
pl
icative
d
eve
l
o
p
ments re
q
uire s
p
ecia
l
forms of nutrition.
4
.1 Artificial feedin
g
A
rtificial feedin
g
is indicated when the liver
p
atient
(
1
.)
i
s no longer abl
e
to, (
2
(
(
.) does not
w
an
t
to, or (
3
.)
i
sno
t
allowed to eat anything because of certain complica-
t
ions. It ma
y
also be necessar
y
to
p
revent malnutrition
as well as to eliminate manifest dietar
y
deficits ra
p
idl
y
and successfully. • Art
i
f
i
c
i
al feed
i
ng can be performed
enterally
b
y nasogastric tubes, percutaneous-endoscopi
c
g
astrotom
y(
PEG
)
or
j
e
j
unostom
y(
PEJ
)
,an
d
p
arenter-
ally
b
y
central-venous catheter s
y
stems. Th
i
s measure
is
carr
i
ed out
sh
ort term
d
ur
i
ng
i
npat
i
ent treatment o
r
l
on
g
te
rm on an outpatient basis at home
.
4.1.1 Enteral feed
i
n
g
Should art
i
f
i
c
i
al feed
i
ng be necessary, the enteral route
o
fa
pp
lication should be
g
iven
p
reference. This is feas-
ible in 90% of he
p
atolo
g
ical
p
roblem cases. Nutritio
n
cons
i
sts of h
i
gh or low molecular we
i
ght formula d
i
ets
.
F
eed
i
ng may be cont
i
nuous or
i
n four to f
i
ve phases.
N
aso
g
astric tubes
(
i.e. 7
⫺
8C
h)
are
h
arm
l
ess even w
h
en
o
eso
p
ha
g
eal varices exist. The correct
p
osition has to be
checked and documented, preferably us
i
ng rad
i
ology! •
A
rt
i
f
i
c
i
al enteral feed
i
ng must correspond w
i
th the pr
i
n-
ci
p
les of ener
gy
and metabolism as well as containin
g
v
itamins, electrol
y
tes and trace elements in o
p
timum
8
79
amounts. It must be appropr
i
ate w
i
th regard to th
e
u
nderlying liver disease. • Enteral feeding has significant
tro
p
hic effects on the intestinal mucosa in terms of stim
-
u
lat
i
n
g
local I
g
A
p
roduct
i
on,
i
m
p
rov
i
n
gi
ts
i
nte
g
r
i
t
y
as
a barr
i
er aga
i
nst bacter
i
al translat
i
on, regulat
i
ng the
p
hysiologically adapted intake of nutritional compo
-
n
ents
(
which are subse
q
uentl
y
made available to th
e
l
i
ver
i
na
p
h
y
s
i
olo
gi
cal f
i
rst
p
ass effect
)
as well as steer
-
i
ng secret
i
on and hormone product
i
on. Ser
i
ous meta-
bolic disturbances must be avoided; other complication
s
occur on
ly
rare
ly
.
(
22, 29, 31
)
4.1.2 Parenteral feedin
g
I
ndications for artificial feedin
g
via a central-venou
s
catheter must be cons
i
dered carefully. As a rule,
i
t
is
p
oss
i
ble only for a br
i
ef t
i
me, s
i
nce the appl
i
cat
i
on
p
eriod is limited b
y
several
c
om
p
lications:
(
1
.
)
venous
thrombosis, (
2
(
(
.)
local infection, and
(
3
.)
s
y
stemic infec
-
t
i
on (
i
n the usually
i
mmunocomprom
i
sed l
i
ver pat
i
ent)
.
W
i
th prolonged parenteral al
i
mentat
i
on,
(
4
.
) compl
i
ca
-
tions in the form of various liver dama
g
e must be antici
-
p
ate
d
.
(
28, 42
)
•
The reported frequency of
l
iver damag
e
is
1
5
⫺
100%. This
g
enerall
y
de
p
ends on the duration o
f
p
arenteral feedin
g
, but occasionall
y
the com
p
osition o
f
the
i
nfus
i
on solut
i
on proves to be
i
nappropr
i
ate. La
-
boratory parameters show
i
ncreases
i
n GPT, GOT an
d
γ
-
GT as well as in alkaline
p
hos
p
hatase and bilirubin
.
As a rule, these chan
g
es are reversible; h
o
w
ever, ex
ces
-
si
ve elevat
i
ons, espec
i
ally catheter-assoc
i
ated
i
nfect
i
ons
,
m
ay necess
i
tate the d
i
scont
i
nuat
i
on of parenteral feed
-
i
n
g
. Deaths have occurred in u
p
to 3% of cases.
(
20, 21
,
23, 27
)
•
V
arious forms o
f
mor
ph
o
l
ogica
ll
iver
d
amage
m
a
y
develo
p
,
p
oss
i
bl
yi
n comb
i
nat
i
on:
1
.
C
holan
gi
t
i
s 6. F
i
bros
i
s
2
. Cholelithiasi
s
7
.
H
epato
/
sp
l
enomega
ly
3. C
h
o
l
estas
i
s
8
.Jau
n
d
i
ce
4.
C
hron
i
che
p
at
i
t
i
s9.L
i
ver c
i
rrhos
i
s
5. Fatt
y
l
i
ver d
i
sease 10.
S
teatohe
p
at
i
t
i
s
Th
e
p
atho
g
enet
i
c mechan
i
sm
s
o
fl
i
ver d
i
sease caused b
y
art
i
f
i
c
i
al feed
i
ng are not fully understood. Var
i
ou
s
th
e
-
o
ri
es
h
ave been postulated:
(
1
.
) deficiency of essentia
l
fatty acids or essential phospholipids, (
2
(
(
.
)
exceedin
g
the
max
i
mum
g
lucose ox
i
dat
i
on rate,
(
3
.)
lack of
i
m
p
ortan
t
s
ubstances (e.g. chol
i
ne, taur
i
ne, glutam
i
ne,
i
nos
i
tol
,
carnitine), (
4
.) in individual cases, the presence of toxi
c
metabolic com
p
onents
(
e.
g
. methionine,
p
lant sterols
)
or newl
y
formed b
i
otoxometabol
i
tes. • It must be borne
i
nm
i
nd that c
i
rrhos
i
spat
i
ents usually show endogenou
s
h
y
perinsulinaemi
a
.
A high intake of glucose should thu
s
be avoided, as should the additional administration of
i
nsul
i
n.
•
The so
-
called
s
u
g
ar su
b
st
i
tute
s
(
e. g. sor
b
ito
l,
m
annitol, xylit, maltit) are not to be recommended.
(
26)
(
s.
p
. 387
)
Ch
a
p
ter 4
0
T
he calculated glucose requ
i
rement of the bra
i
n
i
s 1.5
m
g/kg BW per minute (i. e. 140
⫺
1
60 g carbohydrates
,
560
⫺
700
k
ca
l)
.B
l
oo
dgl
ucose an
dl
actate
l
eve
l
s must
b
e
m
on
i
tored. Fats are the most
i
m
p
ortant ener
gy
carr
i
ers;
20
⫺
5
0% of the total calor
i
e requ
i
rement should be pro-
vided in the form of lipids, preferably as MCT/LC
T
emulsion
(
1
g
fat/k
g
BW
)
. The latter are also readil
y
m
etabol
i
zed b
y
c
i
rrhos
i
s
p
at
i
ents
.
(
2
5
⫺
27
)
In acute l
i
ve
r
f
ailure
,
disturbances in amino-acid metabolism ofte
n
occu
r
.
Amin
o
-
ac
i
d
inf
us
i
o
n
ss
h
ou
l
dbea
v
o
i
ded
in
t
hi
s
ph
as
e
⫺
c
oma-ada
p
ted or l
i
ver-ada
p
ted am
i
no-ac
i
d
i
nfus
i
ons may be
i
nd
i
cated (0.4 g AA/kg BW/day w
i
t
h
a
possible dose increase up to 1.0 (
⫺
1
.5) g/kg BW/day)
.
Vitamins, electrol
y
tes and trace elements must be suffi-
ci
entl
y
subst
i
tuted. The ad
j
uvant use of essent
i
al
p
hos
-
p
hol
i
p
i
ds and orn
i
th
i
ne aspartate
i
s pharmacolog
i
call
y
p
lausible. The regimen of parenteral nutrition must b
e
m
onitored dail
y.
(
23, 26
)
T
he daily requirement of energy, substrate and electro-
ly
tes is based on fixed values.
(
s. tab. 40.5
)
W
ate
r
25
ⴚ
4
5 ml/k
g
B
W
Ener
g
ie
2
5
ⴚ
30
kca/k
g
B
W
앫
Car
b
o
hyd
rat
e
50
ⴚ
5
5
%
앫
Li
p
id
s
30
ⴚ
35
%
앫
Prote
i
n
15
ⴚ
20
%
앫
Standard 0.
8
ⴚ
1
.5 kca/kg B
W
E
l
extro
ly
te
s
⫺
Natr
i
um 550 m
g
⫺
C
hlor
i
d
e
830
m
g
⫺
P
otass
i
u
m
2
,
000
m
g
⫺
C
alcium
1
,
000
m
g
⫺
Ph
os
ph
orus 700 m
g
⫺
M
a
g
nesium 400 m
g
T
a
b
.
4
0.5: Da
i
l
y
re
q
u
i
rement of water, ener
gy
and electrol
y
tes
u
nder normal cond
i
t
i
ons
4
.
2Di
et
in m
a
ln
ut
ri
t
i
o
n
Chron
i
cl
i
ver d
i
seases, espec
i
ally c
i
rrhos
i
s and alcohol
-
i
nduced conditions, are accompanied by (protein-calo
-
ric
)
malnutrition in 6
5
⫺
9
0% of cases. The
p
ro
g
nosis of
the l
i
ver d
i
sease lar
g
el
y
de
p
ends on the nutr
i
t
i
onal stat
e
⫺
t
here
i
s also a d
i
rect relat
i
onsh
i
p between the degre
e
of malnutrition and the progression of the disease and
/
or com
p
lications as well as the
p
robabilit
y
of surviva
l
a
fter l
i
ver trans
p
lantat
i
on
.
(
22, 23, 25, 26, 3
1
⫺
3
4, 36, 39)
•
A
BMI o
f
less than 20.5 denotes malnutrition.
C
auses of malnutrition include:
(
1
.
)
reduced
q
uantit
y
and quality of nutrition, (
2
(
(
.) mald
i
gest
i
on and malab-
sorpt
i
on, (
3
.) accelerated prote
i
n breakdown and pro
-
te
in l
oss as
w
e
ll
as
re
d
uce
d
protein s
y
nt
h
esis
,(
4
.)
increased ener
gy
re
q
uirement, es
p
eciall
y
in the case of
compl
i
cat
i
ons, and
(
5
.
) metabol
i
cd
i
sturbances (e.g.
880
i
nsul
i
nres
i
stance, sympath
i
coton
i
a, loss of metabol
ic
e
fficiency). (s. p. 765)
Th
e
resting energy expenditure
(
REE) (in kcal) i
n
chronic liver disease can be calculated accordin
g
to th
e
H
arris-Bene
d
ict e
q
uatio
n
(
1918
)
, cons
i
der
i
n
g
the
pat
i
ent’s body we
i
ght, kg (W), he
i
ght, cm (H) and age,
years (A). • Multiplying the REE (kcal) by activity
facto
r
1.
2
⫺
1
.4
g
ives the ener
gy
re
q
uirement under nor-
mal da
i
l
y
cond
i
t
i
ons
(i
ne.
g
. trauma, s
p
ort u
p
to facto
r
6
.0 or even more)
.
Me
n
ⴝ
6
6
.
47
ⴙ
(
13.7 ⴛ W
)
ⴙ
(
5.
0
ⴛ
H)
ⴚ
(
6.
8
ⴛ A
)
W
ome
n
ⴝ
6
55.
1
ⴙ
(
9.6 ⴛ W
)
ⴙ
(1.
8
ⴛ
H)
ⴚ
(4.7 ⴛ A
)
Th
e
p
roportions
o
f carbohydrates (4.
0
⫺
5
.0), fat
s
(
1.
0
⫺
2
.0
)
and
p
roteins
(
0.8⫺1.5
)(
each in
g
/k
g
BW/da
y)
i
n
p
at
i
ents w
i
th chron
i
cl
i
ver d
i
sease corres
p
ond t
o
t
hose of an ord
i
nary d
i
et; the bas
i
c calor
i
e requ
i
rement
i
s
2
5
⫺
30 kcal/kg BW/day. • From the metabolic view-
p
oint, and in the case of diabetes, dail
y
food
in
ta
k
e
should be d
i
v
i
ded
i
nto three ma
i
n meals and two snacks
.
A
s a prophylact
i
c measure,
i
t
i
sadv
i
sable to restr
i
ct the
use o
f
co
mm
o
n
sa
l
tto
7
⫺
8
g (because of the very high
N
aCl content in the usual diet
)
. Moreover, a
p
re
p
onder-
ance of lactove
g
etar
i
an
p
rote
i
ns over
p
rote
i
ns der
i
ve
d
from meat and f
i
sh (w
i
th the
i
rh
i
gher product
i
on o
f
ammonia) is recommended. A sufficient intake of vita
-
mins, electrol
y
tes, trace elements and rou
g
ha
g
e should
b
e
g
uarantee
d
.
(
29, 35, 37, 40, 41
)
(s. p. 765
)
P
rincip
l
es o
fl
i
f
est
yl
e
1
.
Al
co
h
o
l
abst
in
e
n
ce
2
.
Av
o
i
da
n
ce o
fn
o
x
ae a
n
dto
xin
s
3. Reach
i
n
g
and ma
i
nta
i
n
i
n
g
a normal BMT
4
.Pay
i
ng attent
i
on to the sens
i
t
i
ve water-electrolyte
balance (s. figs. 16.1, 16.3) (s. pp 294, 311, 765)
5.
Av
o
i
da
n
ce o
fm
a
ln
ut
ri
t
i
o
n
a
n
du
n
de
rn
ou
ri
s
hm
e
n
t
(
s.
pp
604, 751
)
L
ist o
f
i
n
st
r
uctio
n
s:
T
hese “
p
rinci
p
les of lifest
y
le”
should be closel
y
observed b
y
the
p
at
i
ent; the
y
a
pp
l
y
t
o every l
i
ver d
i
sease. We have always
i
ncluded thes
e
p
rinci
p
les on
a
list o
f
instructions
g
iven to our
p
atients
t
o
g
ether with th
e
documentation sheet
.(
s. fi
g
. 15.3
)
4
.3 S
p
ecial diet
s
S
p
ec
i
al d
i
etar
y
measures are of ma
j
or, often even o
f
dec
i
s
i
ve
i
mportance for several types of l
i
ver d
i
sease or
associated com
p
lications. • Here, too, the false, universa
l
c
l
a
im
t
h
at
“
t
h
e
r
e
i
s
n
o
liv
e
r
d
i
et
”i
s
inv
a
li
d.
In
t
h
esa
m
e
w
ay that treatment of a l
i
ver cond
i
t
i
on
i
s
i
ndeed pos-
s
i
ble, there are also d
i
etary measures for certa
i
n forms
o
r com
p
lications of liver disease. • After an exact dia
g-
